Diagnosis
(Page 7)
The Decisions
Waiting for a surgery date at VGH, it seemed prudent to do some research, get educated, and dig a little deeper into my condition. I knew very little about my heart, or what all the terminology meant. But Google was my friend and before long I was knee-deep into finding all I could about ‘Bicuspid Aortic Valve with Severe Aortic Stenosis and a Dilated Ascending Aorta’. The information was overwhelming, but the most important question was: what was the best procedure for someone my age (age 47)?
Although no longer active, one of the first sites I came across that mirrored my condition was from Tonya Henderson-Meyer. She was diagnosed with ‘Bicuspid aortic valve with aortic stenosis and ascending thoracic aortic aneurysm’ and thus worked through many decisions I was about to face. The site was not only informative, but also inspirational, leading me to more research about my condition, and more importantly, my options. The choices I made, I would literally have to live with for the rest of my life, and therefore this was the perfect time to understand what I was up against.
From what I discovered, there were several surgical procedures to choose from — each with their own advantages and drawbacks. One of the first on the list was ‘The Ross Procedure’.
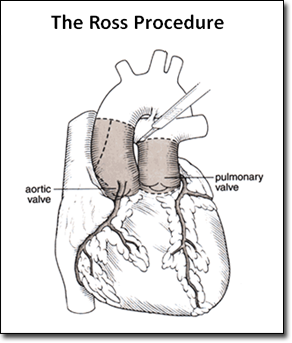
The Ross Procedure
The Ross Procedure is a type of specialized aortic valve surgery where the patient's diseased aortic valve is replaced with his or her own pulmonary valve. The pulmonary valve is then replaced with cryopreserved cadaveric pulmonary valve. In children and young adults, or older particularly active patients, this procedure offers several advantages over traditional aortic valve replacement with manufactured prostheses.
Longevity of the pulmonary autograft in the aortic position is superior to bioprostheses such as porcine valves, which tend to degenerate after only a few years in patients under 35 years of age. Furthermore, anticoagulation is not required as with mechanical valves. Thus, individuals can lead an active life without the risks associated with anticoagulation therapy. This is especially important for women of child bearing age needing aortic valve replacement, as anticoagulation is contraindicated in pregnancy.
Reference: wikipedia.org/wiki/Ross_procedure
Although I wasn’t too concerned about pregnancy, I found very little information on The Ross Procedure, whether surfing the Internet or discussing it with the medical staff. From what I could find, the surgery seemed excessive, and I quickly dismissed it in favor of more traditionally accepted procedures. What everyone was talking about was an aortic valve replacement — with either a mechanical or a biological (live tissue) valve — even though repairing my bicuspid aortic valve disease was also a possibility.
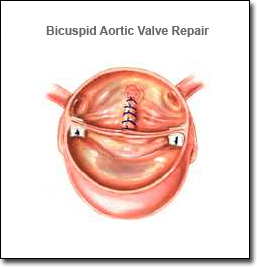
Bicuspid Aortic Valve Repair
Aortic valve repair may be an option for patients who have bicuspid aortic valve disease or other aortic valve conditions that are associated with valve regurgitation (leaking valve). Aortic valve repair is performed less often and is more technically difficult than mitral valve repair. However, the majority (two-thirds), of leaky bicuspid aortic valves can be repaired with good results.
Advantages:
- Preserved heart muscle strength, and preserved natural heart anatomy
- Decreased risk of infection
- Decreased need for life-long anticoagulant medication
Drawbacks:
- This type of aortic valve surgery is technically difficult.
- Aortic valve repair is only an option for leaky aortic valves, not stenotic valves.
- Although a repaired valve can possibly last a lifetime, about 20 to 25 percent of patients will require a valve replacement within ten years. In the best case scenario, the repaired aortic valve will function like the original well-functioning bicuspid valve.

Aortic Valve Replacement (Mechanical)
Mechanical valves are made totally of mechanical parts that are tolerated well by the body. They are made of metal or carbon, and are designed to perform the functions of the patient’s native valve. The bileaflet valve is the most common type of mechanical valve, and consists of two carbon leaflets in a ring covered with polyester knit fabric.
Advantages:
- Mechanical valves are very durable and are designed to last a lifetime.
- Re-operations for mechanical failures or tissue in-growth are uncommon.
Drawbacks:
- Due to the artificial material involved, patients who receive a mechanical valve replacement need to take an anticoagulant medication for the rest of their lives. Anticoagulant medications (blood thinners such as warfarin or Coumadin) delay the clotting action of the blood. Anticoagulants help prevent clots from forming on the replaced valve to reduce the risk of a heart attack or stroke.
- Some patients who have a mechanical valve replacement report a valve clicking noise at times. This is the sound of the valve leaflets opening and closing.
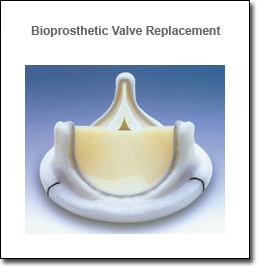
Aortic Valve Replacement (Bioprosthetic)
Biological valves (also called tissue valves) are made of tissue, but they may also have some artificial parts to give the valve support and aid placement. Biological valves may be made from cow tissue (bovine), pig tissue (porcine), or pericardial tissue from other species.
Advantages:
- Most patients who receive a biological valve replacement do not need to take life-long anticoagulant therapy after surgery, unless they have other conditions (such as atrial fibrillation) that require these medications.
Drawbacks:
- Studies on the PERIMOUNT pericardial valve have shown that in a 40-year-old patient, these valves have a 50 percent chance of lasting 15 years or longer, without decline in function. In younger patients, these valves will not last as long, but will still last longer than previous generations of bioprostheses. In older patients they will last longer. The durability of present generation pericardial valves and homografts are very similar.
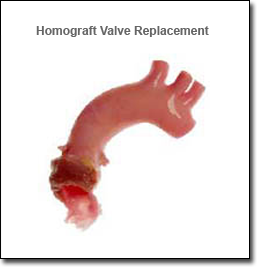
Homograft (or allograft) Valve Replacement
A homograft is an aortic or pulmonic valve that has been removed from a donated human heart, preserved, antibiotic-treated, and frozen under sterile conditions. A homograft may be used to replace a diseased aortic valve, or it may be used to replace the pulmonic valve during the Ross procedure.
Advantages:
- Homografts are ideal valves for aortic valve replacement, especially when the aortic root is diseased or endocarditis (infection) is present.
- Homograft is the best and safest option for patients with severe infections causing aortic valve and root destruction, and abscesses. This is particularly true if the infected valve is a prosthetic valve.
- Homograft valves are well-tolerated by the body because they are most like native valves.
- Most patients who receive a homograft valve replacement do not need to take life-long anticoagulant therapy after surgery, unless they have other conditions (such as atrial fibrillation) that require these medications.
Drawbacks:
- The availability of homografts can be a drawback. In addition, this type of valve replacement surgery is technically difficult. Homograft valves are expected to last about 15 to 20 years. Like bioprosthetic valves, homografts are not as durable in younger patients.
Reference: Cleveland Clinic - Aortic Valve Surgery in the Young Adult Patient
The more I researched, the more complicated the choices got. There was even a possibility of replacing my aortic valve via a Minimally Invasive procedure using a small incision (3 to 4 inches instead of the typical 6 to 8 inches). As with the others, there were advantages and drawbacks, but in the end it was all becoming more overwhelming than helpful. What I needed was to discuss all the options with a surgeon who could shed some light into what my best options were.
And so as my surgery date neared, I prepared an arsenal of intelligent questions that I was about to unleash on the surgeon once I got to VGH and was granted a consultation.